The History of Abortion Law in the United States

Written by Carrie N. Baker, based on previous versions by Marlene Gerber Fried, Laura Kaplan and Susan Yanow, and edited by Christine Cupaiuolo and Laura R. Prieto
The right to abortion has been both supported and contested over time. Abortions occur whether they are illegal or not, but legal bans and practical barriers make the procedure less safe medically, and dangerous in other ways as well. Law and policy can have steep, even deadly, consequences for those seeking abortions.
This article provides an overview of the long history of abortion law in the United States, including key state laws, federal laws, Supreme Court rulings, and their effects.
The First Abortion Laws: Before the 1930s
Social and legal rules governing abortion date back to the colonial period. In the British colonies, abortion was legal before “quickening,” the point at which a pregnant person feels the fetus move, generally at around four or five months.
States did not start prohibiting abortion until the 1820s. These early laws were ambiguous and not strictly enforced. Some laws were poison-control measures, drafted to stem the sale of chemical mixes used to induce abortion. Most initial anti-abortion laws intended to protect pregnant women from coercion or harm.
The history of abortion law intertwines with the histories of racism and slavery. Slavery as a system subjected enslaved people almost entirely to the rule and will of slaveholders. State laws dictated that the children of enslaved mothers were also enslaved. Slaveholders sought to benefit economically and to increase their labor force, so they used their power to compel enslaved people to have as many children as possible. Enslaved women resisted as best they could. They privately used traditional knowledge to control their fertility, including herbal methods of contraception and abortion, despite the risk of punishment. Slavery’s intense hardships and violence shaped Black people’s lives for generations after emancipation.
By the late 19th century, most states had passed laws restricting abortion. Such laws enabled men in the newly established medical profession to take over the highly profitable business of childbirth from midwives, whom they condemned for performing abortions. It was also part of a backlash against the growing women’s rights movement, which did not vocally support abortion but advocated for “voluntary motherhood.” Birth control of any sort was seen as a threat to male dominance; Restricting abortion became part of an effort to control women and confine them to a traditional childbearing role.
Additionally, attacks on abortion access in the late 1800s were rooted in white supremacy, racism, and anti-immigrant stigma. The eugenics movement sought to control reproduction in order to breed a superior human race. They cited comparatively higher Black and immigrant birth rates to raise fears that others would soon outnumber and dominate native-born white Americans. The drive to criminalize abortion thus pointed to increased immigration, specifically of Catholic and Jewish immigrants, and the declining birthrate among U.S.-born white Protestant women. The birth control movement sometimes used eugenic arguments in favor of contraception as well.
The Toll of Illegal Abortions
Despite the laws against them, people continued to seek and have abortions. Many factors – your finances, your race, and where you lived – affected your chances of finding an abortion provider. Women with money could sometimes find a physician in the United States who would perform the procedure for a high fee. By the mid-20th century, some women obtained abortions by traveling to other countries where the procedure was legal. Those without funds, especially women of color, suffered disproportionately. They were often at the mercy of incompetent practitioners with questionable motives or forced to resort to dangerous self-abortions.
In desperation, some women inserted knitting needles or coat hangers into their vaginas and uteruses, douched with solutions such as lye, or ingested strong drugs or chemicals. Because many deaths were not officially attributed to unsafe, illegal abortion, it’s impossible to know the exact number of lives lost. However, we do know that thousands of women a year were treated for health complications due to botched, unsanitary, or self-induced abortions. Many of those women died. Others suffered from infertility, chronic illness, and pain.
Hospitals had entire wards dedicated to caring for women suffering from health complications, most of whom had tried to induce their own abortion or had had an illegal abortion. In 1939, Cook County Hospital, Chicago’s public hospital, reported treating more than 1,000 women annually. That number increased to nearly 5,000 in 1962. One medical provider recalled the experience:
In 1972 I was a third-year medical student doing my first clinical experience in obstetrics and gynecology.... At that time, Cook County had a 40-bed Septic Abortion Ward. It was a large room with the beds separated by curtains. The role of the medical student — my role for the week I was there — was to push a large cart of antibiotic solutions around the room, hang the antibiotics and connect them to the IV line, and take the patients' vital signs. When one of the patients died, I was to call the diener — the morgue attendant who collected the bodies. A death in this ward was a common occurrence.

Making Illegal Abortion Safer
Wherever abortion is illegal, caring and dedicated people take enormous risks to provide safe abortions clandestinely, to treat people who have complications, and to help them find safe providers.
Before the Supreme Court’s landmark Roe v. Wade decision that legalized abortion in 1973, some well-trained physicians and other medical practitioners risked imprisonment, fines, and loss of their medical licenses to provide abortions. Information about these services often spreads by word of mouth.
Groups formed to connect pregnant people to trusted abortion providers. For instance, in the late 1960s, the Clergy Consultation Service on Abortion — a network of concerned pastors and rabbis — set up referral services to help women find safe illegal abortions.
Feminist groups formed their own independent referral groups as well. In Chicago, a group of trained laywomen called the Abortion Counseling Service of the Chicago Women’s Liberation Union went even further, creating an underground feminist abortion service in 1969. The group, whose code name was Jane, provided safe, inexpensive, and supportive illegal abortions. Over a four-year period, the group provided more than 11,000 first- and second-trimester abortions with a safety record comparable to that of today’s legal medical facilities.
Laura Kaplan, a former Jane member and the author of The Story of Jane: The Legendary Underground Feminist Abortion Service, describes the women involved:
We were ordinary women who, working together, accomplished something extraordinary. Our actions, which we saw as potentially transforming for other women, changed us, too. By taking responsibility, we became responsible. Most of us grew stronger, more self-assured, confident in our own abilities. In picking up the tools of our own liberation, in our case medical instruments, we broke a powerful taboo. That act was terrifying, but it was also exhilarating. We ourselves felt exactly the same powerfulness that we wanted other women to feel.
Organizing to Change the Law
In the 1960s, inspired by the civil rights and antiwar movements, women organized a women’s liberation movement. Reproductive rights were among their highest priorities.
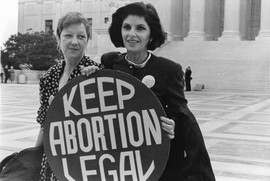
Advocates marched and lobbied to make abortion safe and legal. At speak-outs, women publicly shared their illegal abortion experiences for the first time. These events demonstrated that millions of people were willing to break the law and risk their lives to obtain an abortion, or to help someone else to do so. The movement also connected abortion rights to gender equality.
When I was 15 and pregnant, abortion was illegal. I was denied any choice—I had a baby that I gave up for adoption. This experience has been a driving force in my life. I became an OB/GYN; I do abortions because I am totally committed to making sure that other women have the options that I didn’t have.
Between 1967 and 1973, 14 states modified their restrictive abortion laws and four states completely repealed their laws. The revised laws typically allowed access to abortion only in certain circumstances, such as when the pregnancy was the result of rape or incest.
In 1967, Colorado became the first U.S. state to decriminalize abortion, although only in cases of rape, incest, or when the pregnancy would cause “permanent physical disability” to the woman. In 1970, Hawaii legalized abortion through 20 weeks for residents of that state. New York became the first state to legalize abortion on demand through the 24th week of pregnancy. Washington, D.C., also allowed abortions. Two other states, Alaska and Washington, followed the same year. During this period, women who could afford it began traveling to places where it was legal to get abortions.
Feminist networks offered support, loans, and referrals to those who needed abortions, and they fought to keep down the cost of the procedure. But for every person who managed to get to a state where abortion was legal, many others with limited mobility, and who could not afford to travel, still sought illegal abortions.
Roe v. Wade: A Milestone Decision
On January 22, 1973, the U.S. Supreme Court’s landmark Roe v. Wade decision struck down all existing criminal abortion laws. The Court ruled that people have a fundamental “right of privacy … founded in the Fourteenth Amendment’s concept of personal liberty.”
The Court weighed a pregnant person’s right to privacy against the state’s interests in supporting maternal health and fetal life. The Court held that the abortion decision must be left to the person carrying the pregnancy, in consultation with their doctor, during the first trimester; that the state may regulate abortion in ways that are reasonably related to maternal health in the second trimester; and that the state may regulate or prohibit abortion in the third trimester, except where necessary to preserve the person’s life or health.
Weakening the Constitutional Protection for Abortion
While many were thrilled and relieved that abortion was now legal across the country, others were appalled and turned to state legislatures to restrict access. Upon the Roe decision, abortion became a partisan issue. The Republican party adopted an anti-abortion position, whereas the Democratic party supported abortion rights. Soon abortion became a major wedge issue for white evangelical Christians, who mobilized to restrict abortion access and aligned politically with the Republican party. This change in rhetoric and policy has been traced to their need for a successful uniting issue after their support for racial segregation became less feasible as a wedge issue.

From 1973 until 1992, restrictions on abortion were passed in almost every state. Abortion rights activists appealed, but the Supreme Court rejected hearing most of these cases. In fact, during this time period the Court handed down several major rulings that made it more difficult for young people and those with limited funds to access abortion.
Bellotti v. Baird and Parental Consent
In Bellotti v. Baird (1979), the Supreme Court ruled that states could require that minors obtain parental consent for an abortion. The Court, however, said that states must provide a judicial bypass option, whereby young people could petition a judge for permission to obtain an abortion without notifying their parents – if they could show that they were mature enough to make their own decision or that the abortion was in their best interests.
Parental consent laws discouraged many minors from even seeking legal abortions. The first person known to die as a result of these laws was seventeen-year-old Rebecca (Becky) Bell of Indiana. Bell had an illegal abortion because of the state’s parental consent law. Complications from the septic abortion led to her death on September 16, 1988.
In addition to permitting various restrictions like parental consent, the Supreme Court also allowed Congress to block Medicaid funding for abortion. When Roe v. Wade legalized abortion, Medicaid — a healthcare program funded jointly by the federal government and individual states — covered abortion care as part of comprehensive health care services provided to low-income women.
Parental consent laws discouraged many minors from even seeking legal abortions. The first person known to die as a result of these laws was seventeen-year-old Rebecca (Becky) Bell of Indiana. Bell had an illegal abortion because of the state’s parental consent law. Complications from the septic abortion led to her death on September 16, 1988.
In addition to permitting various restrictions like parental consent, the Supreme Court also allowed Congress to block Medicaid funding for abortion. When Roe v. Wade legalized abortion, Medicaid — a healthcare program funded jointly by the federal government and individual states — covered abortion care as part of comprehensive health care services provided to low-income women.
Hyde Amendment and Medicaid Funding
Then in 1976, Congress passed the Hyde Amendment, which banned the use of federal funding for abortion care, except in limited cases. Most states followed, instituting bans in their state Medicaid programs.
Because so many women depend upon Medicaid for their health care, the Hyde Amendment effectively made it much more difficult for low-income women — disproportionately women of color — to get abortions. Rosie Jiménez became the first person known to die as a result of the Hyde Amendment. Jiménez was a nursing student in Texas and the mother of a 4-year-old girl. Unable to use Medicaid to afford a safe medical abortion in the U.S., she underwent the procedure in Mexico instead. A resulting infection spread through her body. Jiménez died days later, on October 3, 1977.
In 1980, in Harris v. McRae, the Supreme Court upheld Hyde in a narrowly divided ruling, stating that women’s constitutional rights are not violated by the ban on federal funding for abortions, even if the abortion is medically necessary for a person’s health.
Planned Parenthood v. Casey: A New Legal Test

The next major Supreme Court ruling regarding abortion access came in 1992, when the Court, in Planned Parenthood v. Casey, considered a highly restrictive Pennsylvania law that required a 24-hour waiting period, spousal notification, parental consent, a mandate that doctors give biased counseling to people seeking abortion health care, and burdensome reporting requirements.
In its decision, the Court abandoned the trimester framework and created a new legal test for allowable restrictions.
Before viability — which is the point at which a fetus can survive outside the womb, somewhere between 24 and 28 weeks — the Court allowed restrictions on abortion, as long as the law does not place an “undue burden” on a person’s access to abortion. The Court defined an “undue burden” as a restriction that has the “purpose or effect of placing a substantial obstacle in the path of a woman seeking an abortion.”
Under this new standard, the Court upheld all of the Pennsylvania restrictions except for spousal notification, which it noted could place women in danger from abusive husbands.
The Court allowed states to ban abortion after viability, as long as they had an exception to preserve the life or health of the pregnant person.
Stenberg v. Carhart and Second-Trimester Abortions
In the aftermath of Casey, state and local legislatures began to pass more laws to restrict abortion, and the Supreme Court more often upheld them.
In the 2000 case of Stenberg v. Carhart, the Supreme Court struck down a Nebraska statute prohibiting what anti-abortion advocates called “partial birth abortion.” Although the term does not refer to any medical procedure, the law was interpreted as prohibiting doctors from performing an intact dilation and extraction abortion, a procedure sometimes used for second trimester abortions.
The Court held that if a particular abortion method may be safer in some circumstances, the state cannot flatly ban the method and must allow a maternal health exception.
Anti-abortion rights advocates deliberately used “partial-birth abortion” to confuse the public and build support for restrictions.
Three years later, Congress passed nearly identical legislation, the Partial-Birth Abortion (PBA) Ban Act of 2003, which was signed into law by President George W. Bush. The PBA Ban Act is one of many instances of politicians dictating the practice of medicine without regard for medical science or a pregnant person’s health.

Gonzales v. Carhart Changes Course
Abortion rights advocates challenged the PBA Ban Act again in 2006. As a result, the Court overruled Stenberg v. Carhart and upheld the abortion ban in the case of Gonzales v. Carhart (2007).
Gonzales v. Carhart highlights the increasing politicization of the Supreme Court. The ruling was 5 to 4, with two newly appointed conservative justices (John Roberts and Samuel Alito) in the majority. Republican presidents would consider only anti-abortion candidates as viable nominees for the Supreme court..
In her dissent to Gonzales v. Carhart, Supreme Court Justice Ruth Bader Ginsburg criticized the ruling. She wrote:
Today’s decision is alarming … It tolerates, indeed applauds, federal intervention to ban nationwide a procedure found necessary and proper in certain cases by the American College of Obstetricians and Gynecologists (ACOG). It blurs the line, firmly drawn in Casey, between previability and post-viability abortions. And, for the first time since Roe, the Court blesses a prohibition with no exception safeguarding a woman’s health.
The Rise of State Restrictions
According to Guttmacher Institute, states passed more than 1,300 abortion restrictions between the 1973 Roe v. Wade decision and June 2022. These laws ban abortion after a particular gestational age or based on sex, race, or genetic anomaly, prohibit specific abortion methods, impose biased counseling and waiting periods, require unnecessary ultrasounds, restrict access to medication abortions, limit who can provide abortion health care, and impose targeted regulation of abortion providers, or TRAP, regulations.
The constant onslaught of abortion restrictions endangers women’s health. It also forces reproductive rights and justice activists to challenge each individual restriction and fight the same battles repeatedly.
TRAP Regulations Take Hold
TRAP (Targeted Regulations of Abortion Providers) regulations refer to burdensome and medically unnecessary requirements that are more stringent than requirements for other medical procedures of similar risk.
For example, TRAP laws sometimes mandate the width of hallway corridors in abortion facilities -- forcing clinics to close if they can’t afford expensive renovation costs. TRAP laws can also require physicians to obtain admitting privileges at a nearby hospital. But hospitals’ religious affiliations, or their refusal to involve themselves in a politically charged issue, leave doctors with no hospitals willing to grant them admitting privileges in some areas.
Anti-abortion rights activists claim the requirements make abortion safer, but there is no evidence that greater safety results. To be clear, abortion is one of the safest medical procedures in the country, far safer than pregnancy and childbirth, and complications are rare.
The true intent of TRAP laws is not to improve the safety of abortion but to place expensive and complex rules on clinics and abortion providers so that they have to shut down.
Whole Woman’s Health v. Hellerstedt: Challenging TRAP Laws
In 2016, a TRAP law challenge finally reached the Supreme Court in the case of Whole Woman’s Health v. Hellerstedt (2016). The case involved a Texas law that 1) required physicians who perform abortions to have admitting privileges at a nearby hospital; and (2) required abortion clinics in the state to have facilities comparable to an ambulatory surgical center – which usually means a freestanding surgery center with an operating room.
The Court ruled that these restrictions violated the 14th Amendment because they imposed an undue burden on abortion access. The Court said that reviewing courts must “consider the burdens a law imposes on abortion access together with the benefits those laws confer,” and that courts retain “an independent constitutional duty to review factual findings where constitutional rights are at stake.”
Texas tried to justify the restrictions on the grounds of protecting women’s health, but evidence in the record proved that the provisions provided no medical benefit and in fact endangered women.
Nevertheless, according to Guttmacher Institute, as of August 2023, 23 states had TRAP laws or policies in place.
Personhood Laws
Those who oppose reproductive rights use the concept of “personhood” to attempt to pass laws that define zygotes, embryos, and fetuses as “persons” separate from the pregnant person, and with the full legal rights of a person.
The goal of personhood laws is to criminalize abortion as well as any forms of birth control that work by preventing sperm from fertilizing an egg. Opponents of abortion rights have even used proposed measures to prevent doctors from treating complicated and potentially dangerous pregnancies.
Alabama, Kansas, Missouri, and several other states have passed laws that use personhood language. Many other state legislatures have also considered personhood language in state laws.
Protection of Patients and Providers
For decades, the anti-abortion rights movement has waged a widespread campaign of harassment, violence and terror against doctors who provide abortions, their staff, clinics and patients. Tactics have included blockades of clinic entrances, facility invasions, property damage, stalking, death threats, and physical violence.
According to a report from 2022, by the National Abortion Federation, anti-abortion extremists have murdered 11 people since 1977. They have committed additional violence against patients, providers, and volunteers through 42 bombings, 196 cases of arson, 491 assaults, and thousands of other incidents of criminal activities.
Anti-abortion violence escalated in the early 1990s. In response, the U.S. Congress (which had a Democratic majority at the time) passed the Freedom of Access to Clinic Entrances Act of 1994. This federal law prohibits intentional property damage and the use of “force or threat of force or … physical obstruction” to “injure, intimidate or interfere with” someone entering a health care facility.
Several states have passed laws to protect patients, providers, and clinics from anti-abortion extremists. As of 2021, 14 states had laws to protect access to clinics, including laws prohibiting blocking an entrance; threatening or intimidating staff or patients; damaging a facility; making harassing phone calls; creating excessive noise outside a clinic; possessing and/or having access to a weapon during a demonstration at a facility; trespassing; or releasing a substance that produces noxious odor on clinic premises.
Several states have laws creating a buffer zone around clinics, or a “bubble zone” around a person within a specific distance of a clinic’s entrance or driveway. In the 2000 decision Hill v. Colorado, the Supreme Court upheld a floating 8-foot “bubble zone” law in Colorado, but in the case of McCullen v. Coakley (2014), the Court struck down a Massachusetts law that placed a 35-foot buffer zone around clinic entrances.
Despite these protections, more than half of all clinics that provided abortion care in 2021 reported experiencing threats and intimidation against doctors and staff.
Abortion and the Affordable Care Act

Prohibitions or restrictions on abortion coverage also extend to statutes governing public funding. In 2010, the Affordable Care Act (ACA) was signed into law, extending the Hyde Amendment restrictions on abortion coverage to states’ newly created health insurance exchanges.
The ACA allows states to prohibit abortion coverage entirely in health insurance plans offered through an exchange. Since the law was implemented, multiple states have barred health plans from covering abortion. The ACA also permits providers and facilities to refuse to provide, pay, or refer for abortion services under federal refusal provisions. As of 2021, 46 states had similar laws.
Abortion advocates continue to fight the Affordable Care Act’s restrictions on insurance coverage for abortion. These restrictions force some people to continue pregnancies they do not want and may put their health or lives at risk.
As more states attempt to limit or ban private insurance coverage for abortion services, organizations including the Center for Reproductive Rights and Guttmacher Institute are pushing to ensure coverage for all pregnancy-related care, including abortion, under the ACA.
Restrictions on Funding Abortion

In addition to restrictive state laws, the federal Hyde Amendment and subsequent federal and state laws banning public funding for abortion continue to limit access for people with low incomes, who are also disproportionately women of color. In May of 2021, President Joe Biden, proposed the first-ever federal budget without the Hyde Amendment, but the Hyde Amendment was restored and passed in March of 2022.
Currently, Medicaid uses federal funds to cover abortion only in cases of rape, incest, or when the pregnant person’s life is endangered by an illness, injury, or physical disorder. States can decide whether or not to use their own funds to cover abortion.
Thirty-three states and the District of Columbia follow the federal standard and only provide abortions in the circumstances outlined in the Hyde Amendment. In 2018, over half of reproductive age women on Medicaid — more than 7 million women — lived in states that restrict abortion coverage.
As of 2022, 16 states fund abortion services on the same terms as other pregnancy-related health services, which means these states use their own funds to cover abortions, in addition to what the Hyde Amendment allows.
The Hyde amendment and the other laws it inspired have expanded in scope over time. Currently, they also limit federal funding of abortion services for federal employees, women in the military and the Peace Corps, American Indian and Alaskan Native women who use the Indian Health Service, and women in federal prisons and immigration detention facilities.
Under the leadership of women of color organizations and their allies, activists are attempting to repeal Hyde and restore public funding for abortion health care.
The Global Gag Rule

Along with prohibiting Medicaid recipients from receiving coverage for most abortion services, Congress has also blocked foreign aid from covering or even providing information on abortion health care. The Helms Amendment — first passed in 1973 and named after the late ultra-conservative Senator Jesse Helms (R-N.C.) — bars the use of U.S. foreign aid funds to support abortion care.
In 1984, Ronald Reagan instituted the Mexico City Policy, which came to be known as the “global gag rule.” Under this rule, foreign nongovernmental organizations are not allowed to receive U.S. family planning funding unless they agree to stop providing abortion-related services or advocating for the expansion of abortion access, using any source of their funding.
Democratic president Bill Clinton ended the global gag rule in 1993 but his Republican successor George W. Bush reinstated it. EveryRepublican president since 1984 has restored the global gag rule, and every Democratic president has removed it. In 2017, Donald Trump expanded the global gag rule to apply to all U.S. global health assistance. President Biden rescinded the global gag rule when he took office in January 2021.
Some members of Congress have fought against these global restrictions on abortion care. In 2019, Sen. Jeanne Shaheen (D-NH) and Rep. Nita Lowey (D-NY) introduced the Global Health, Empowerment and Rights (HER) Act, which would permanently prevent future presidents from reimposingthe global gag rule. And in 2020, Rep. Jan Schakowksy (D-Ill.) introduced the Abortion is Health Care Everywhere Act of 2020, the first-ever legislation to repeal the Helms Amendment.
The Domestic Gag Rule

In March 2019, the Trump administration enacted a domestic gag rule, which prohibits U.S. clinics receiving Title X family planning funds from referring their patients for abortion health care.
For decades, Title X clinics have provided free or low-cost reproductive health care. The domestic gag rule devastated the Title X network’s capacity, cutting it by half. President Biden reversed the domestic gag rule in November of 2021.
To strengthen abortion rights more broadly, advocates are now pushing for the Women’s Health Protection Act, which would prohibit a range of abortion restrictions, including previability bans, state mandates of unnecessary procedures and inaccurate counseling, barriers to telemedicine abortion, TRAP laws, and forcing extra in-person visits to a doctor.
Supreme Court Changes during the First Trump Administration
After Donald Trump became president in 2017, he appointed two ultra-conservative justices to the Supreme Court in his first two years — Neil Gorsuch in 2017 and Brett Kavanaugh in 2018 — emboldening anti-abortion rights activists, policymakers, and right wing, antifeminist judges.
The appointments also emboldened state legislatures. In the first five months of 2019, seven states under Republican control passed bans on first-trimester abortions.
Georgia, Kentucky, Louisiana, Mississippi and Ohio adopted so-called “fetal heartbeat” bills that prohibit abortions after six weeks of pregnancy. Fetuses do not yet have hearts at six weeks of gestation, but six weeks is usually when doctors can start detecting embryonic cardiac activity via ultrasound. Missouri passed an eight-week ban. Alabama voted to ban all abortions except to save a pregnant person’s life, with no exception for rape or incest.
Despite the Whole Woman’s Health v Hellerstedt decision in 2016, the Fifth Circuit Court of Appeals upheld an identical law in Louisiana, requiring doctors to have admitting privileges in a hospital in order to provide abortions.. The Louisiana law hoped to be considered separately from the Texas law at issue in Whole Woman’s Health.
In June of 2020, the Supreme Court narrowly ruled in June Medical Services v. Russo that the Louisiana law was unconstitutional. Chief Justice Roberts, who had dissented in Whole Woman’s Health, concurred in the judgment that struckdown the Louisiana law.
In his opinion, Roberts criticized Whole Woman’s Health and suggested ways to narrow the undue burden standard in future cases, but he concurred on the grounds of respect for precedent. In doing so, Roberts created a blueprint for states to restrict abortion.
In August 2020, Arkansas enacted four new abortion restrictions. One of these, a ban on dilation and extraction procedures, prevented the most common method of providing second-trimester abortion care. Another required that abortion providers notify law enforcement officials when a patient 17 years old or younger seeks an abortion.

Supreme Court’s Lurch to the Right Sparks More State Bans
Shortly before the 2020 presidential election, staunch feminist Supreme Court Justice Ruth Bader Ginsburg died. Despite the imminent election he would soon lose, Donald Trump nominated fundamentalist anti-abortion advocate Amy Coney Barrett to fill Ginsburg’s seat.
The Republican Senate leadership confirmed Barrett’s nomination in record time, tilting the balance of the court to a 6-3 hard right supermajority with the three Trump appointees.
In response to this shift, Republican states quickly began passing anti-abortion laws. According to the Guttmacher Institute, states enacted 108 abortion restrictions in 2021, far surpassing the previous post-Roe record of 89 set in 2011.
In May 2021, Texas passed a six-week abortion ban — called S.B. 8 — with a private enforcement scheme that attempts to circumvent federal court review. S.B. 8 allows private citizens to file civil lawsuits against anyone who knowingly "aids or abets" an abortion. People receiving abortion care are exempt, but a wide range of others can be sued, including abortion providers and clinic staff, friends and family who help the pregnant person with advice or funds, and drivers who take people to their appointments. The law tells the courts to award plaintiffs at least $10,000 in damages from defendants.
Abortion providers challenged the law, but the Supreme Court allowed the ban to go into effect on September 1, 2021, despite the fact that the law clearly violated Roe.
Dobbs v. Jackson Women’s Health Organization: Overturning Roe

On June 24, 2022, the United States Supreme Court ended constitutional protections for the right to abortion. The sweeping decision in Dobbs v. Jackson Women’s Health Organization overturned the longstanding precedents of Roe v. Wade (1973) and Planned Parenthood v. Casey (1992).
Neil Gorsuch, Brett Kavanaugh and Amy Coney Barrett– three Supreme Court justices nominated by President Donald Trump——joined Clarence Thomas and Samuel Alito, who authored the opinion to strike down Roe. (Chief Justice Roberts concurred in the Court’s judgment, but he did not join in the majority opinion overturning Roe.) The Dobbs majority opinion gave three main reasons why it argued that abortion is not a constitutional right: because the Constitution does not explicitly mention abortion, because the framers of the 14th Amendment in 1868 did not intend to protect the right to abortion, and, finally, because abortion rights are not “deeply rooted in the country’s history and traditions.” The Dobbs opinion focused on mid-19th century abortion prohibitions, but ignored the longer history of legal abortion in the United States. Throughout the majority opinion in Dobbs, the Supreme Court repeatedly refers to embryos and fetuses as “unborn human beings.” In a strong dissent, Justices Stephen Breyer, Sonial Sotomayor and Elena Kagan stated:
"Whatever the exact scope of the coming laws, one result of today’s decision is certain: the curtailment of women’s rights, and of their status as free and equal citizens… After today, young women will come of age with fewer rights than their mothers and grandmothers had."
In addition to allowing states to outlaw abortion, the Dobbs decision endangers rights to use in vitro fertilization. It also threatens the right to use IUDs and emergency contraception, because many anti-abortion proponents believe—contrary to scientific evidence—those forms of contraception cause abortion. The sweeping reasoning of the Court puts at risk a range of privacy-based constitutional rights. In his concurrence, Clarence Thomas calls on the court to revisit the Griswold decision guaranteeing access to contraception and Obergefell, which established the right to enter into a same-sex marriage.
As a result of Dobbs, abortion bans went into effect in many states, covering much of the South and Midwest of the United States. The decision thus left about one-third of women nationwide without access to abortion services in their home states. By July 2024, 14 states adopted total bans on abortion and another eight states banned abortion at or before 18 weeks. Most of these bans did not have any exceptions for rape, incest or health threats. Some bans had exceptions to preserve the life of the pregnant woman, but these exceptions were extremely narrow and so vaguely written that few doctors were willing to provide abortion in life-threatening cases for fear of criminal prosecution.
In response to Dobbs, Republican lawmakers and anti-abortion activists from the Susan B. Anthony List announced they were working on legislation to ban abortion nationwide, which they could achieve if Republicans were to win Congress and the White House in 2024. Anti-abortion advocates have also asked the Supreme Court to ban abortion nationwide by ruling that fetuses are persons protected by the Fourteenth Amendment. The Dobbs opinion has repeated references to “unborn humans”—23 times—laying the groundwork for striking down state laws protecting abortion rights in states such as California and New York.
People seeking abortion care and those who help them face criminal prosecution and civil lawsuits in several anti-abortion states. And unlike the time before Roe, we now live in an era of mass incarceration, which makes it far more likely that women will be surveilled, arrested, and jailed.
Even before Dobbs, police and prosecutors were already criminally charging pregnant women for miscarriage, abortion, and pregnancy loss, such as Texas woman Lizelle Herrera, who was arrested in April for murder after allegedly causing her miscarriage. Approximately 1,200 women—who are disproportionately low-income women and women of color—have been prosecuted for their behavior during pregnancy over the last 15 years. The National Association of Criminal Defense Lawyers published a report in August of 2021 warning about the threat of increasing criminalization post-Roe.
The New York-based privacy group Surveillance Technology Oversight Project released a chilling report in June of 2022 detailing how anti-abortion governments and private entities are already using cutting-edge digital technologies to surveil women’s search history, location data, messages, online purchases, and social media activities by using geofencing, keyword warrants, big data, and more.
In the year after Dobbs, at least 210 women faced criminal charges because of their pregnancies or pregnancy outcomes—the highest number of documented prosecutions in a single year. The real number is likely much higher, according to research by Pregnancy Justice. The majority of cases occurred in “states that have enshrined fetal personhood in their civil and criminal laws,” such as Alabama (104 cases), Oklahoma (68 cases) and South Carolina (10 cases)—all states that have near-total abortion bans and some of the worst maternal and infant health outcomes.

In addition to surveillance and criminal prosecution, abortion bans have had devastating effects on the health and well-being of women and their children. Research shows that after people who are denied abortions, they have more serious health problems than people who receive the abortions they seek. In addition, those denied abortions are also more likely to stay in contact with a violent partner.
Those denied abortion care also experience significant, long-term economic hardship and insecurity. Women who were unable to obtain an abortion had financial challenges that continued through all five years of one study. They included a 78 percent increase in unpaid bills and an 81 percent increase in negative credit report notations, such as bankruptcies and evictions, compared with the women who were able to get an abortion. Their children were more likely to experience developmental delays and to live in poverty than the children of women who were able to have abortions.

While reactionary states banned abortion, progressive states such as California, New York and Massachusetts responded to Dobbs by passing laws strengthening abortion rights. As a result, the United States became further divided over access to abortion health.Some states banned abortion while others expanded access to abortion healthcare.
Despite increasing restrictions, the total number of abortions nationally grew from 84,690 in April 2022, to 102,350 in January 2024—a 21 percent increase in less than two years, reported the Society for Family Planning in their August 2024 #WeCount report. Guttmacher Institute reported that one in five patients–171,000 people–had to travel out of state for abortion care in the first half of 2023, compared to one in ten in 2020. Enhanced access to telehealth abortion was a major reason for the increase in abortion.
Telemedicine and Medication Abortion
Telehealth abortion combines medication abortion, which uses pills to end a pregnancy, with telemedicine, which allows health care providers to meet with patients via videoconferencing or telephone consultations.
Medication abortion is a safe way to end an early pregnancy. Approved by the FDA through 10 weeks of pregnancy, medication abortion uses two different medicines: mifepristone, which interrupts the flow of the hormone progesterone that sustains the pregnancy; and misoprostol, which causes contractions. This combination of medications is 95-97 percent effective. Misoprostol alone is also highly effective.
Between 2016 and 2020, the organization Gynuity Health Projects operated a research study on telemedicine abortion called TelAbortion. Participating clinicians in 13 states provided medication abortion care by video conference and mail without an in-person visit. This study proved that telemedicine abortion is safe and effective.
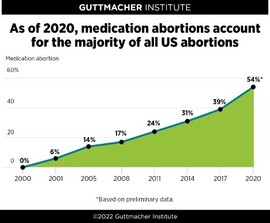
According to Guttmacher Institute, medication abortions accounted for almost two-thirds of abortions in 2023. (The actual rate is likely higher because of the growing number of people who are self-managing their abortions using medication purchased online or obtained in other ways.)
The growth of medication abortion dovetailed with the expansion of telehealth to provide new opportunities for accessing abortion health care. As abortion restrictions increased, and harassment of people entering health clinics persisted, people increasingly turned to medication abortion and telehealth to increase their safety and privacy when obtaining abortion care. A major change in federal policy increased access to telemedicine abortion in December 2021.
State & FDA Policy Restrictions on Telemedicine Abortion
Numerous policy barriers limited the reach of telehealth abortion for years. Many states prohibited patient access to the abortion pill via telemedicine, despite its proven safety. In 2022, 19 states required the prescribing clinician to be physically present when prescribing the abortion pill, while 29 states required the clinician prescribing the abortion pill to be a physician. Neither of these requirements were necessary because the abortion pill is extremely safe and effective.
Another significant barrier to telemedicine abortion until December of 2021 was that the U.S. Food and Drug Administration (FDA) restricted the distribution of mifepristone.
The FDA approved mifepristone in 2000, but pressure from anti-abortion forces led the agency to block easy access to mifepristone, using their Risk Evaluation and Mitigation Strategy (REMS). REMS is a drug safety program that allows the FDA to restrict the circulation of certain medications to help ensure the benefits of the medication outweigh its risks. Under the REMS program, mifepristone had to be dispensed in person at a clinic, medical office or hospital under the supervision of a healthcare provider registered with the drug manufacturer.
In the wake of COVID-19, advocates increasingly challenged the FDA’s REMS restrictions on the abortion pill. This effort was supported by research on the safety of a no-test medication abortion protocol that allows doctors to screen patients by phone or video and then mail abortion pills directly to them.
In March of 2020, a coalition of 21 state attorneys general, led by California Attorney General Xavier Becerra, sent a strongly-worded letter to the U.S. Department of Health and Human Services and its U.S. Food and Drug Administration (FDA), urging the Trump administration to waive or utilize its discretion on enforcement of its REMS designation. Reproductive health groups also pressured the government to remove the REMS restriction on the abortion pill.
That summer, a federal judge in Maryland issued a ruling temporarily suspending enforcement of an FDA restriction on abortion pills during the pandemic. The Trump administration appealed twice to the Supreme Court, which reversed the decision in January of 2021, two months after Trump lost the presidential election.
Under the Biden administration, the FDA reversed course, lifting the in-person distribution requirement on April 12, 2021, for the duration of the pandemic. The Biden administration later announced that the FDA would review the REMS restriction for modification.
In December of 2021, the FDA partially lifted the REMS restriction by removing the long-standing rule that health care providers must distribute the abortion pill mifepristone to patients in person. However, the FDA kept mifepristone within the REMS program, maintaining a requirement that health care providers must register with the drug manufacturer to become certified to prescribe mifepristone. This greatly limits the number of qualified providers.
Another change in the REMS, made it easier for clinicians to prescribe mifepristone, however. The FDA allowed some pharmacies to distribute the drug. But the FDA is still blocking the abortion pill from being available in pharmacies, like any other drug.
And while the partial removal of the FDA REMS restriction opened the door to expanded telemedicine abortion access in many states, 19 states still required in-person distribution of the drug.
Despite ongoing restrictions, use of telehealth abortion grew to 20 percent of all abortions in the formal health care system nationally by March 2024, an increase from 4 percent nationally in April 2022.
After Dobbs
Despite the claims of conservative members of the Supreme Court that Dobbs would “return the issue of abortion to the people’s elected representatives,” the decision spurred a firestorm of state-level litigation that quickly returned the issue once again to the Supreme Court. In November 2022, an anti-abortion group of doctors and a dentist filed a lawsuit against the FDA: Alliance Against Hippocratic Medicine v. FDA. The plaintiffs challenged the FDA’s approval of mifepristone in 2000 and subsequent expansions to access in 2016, 2019 and 2021. The plaintiffs inaccurately claimed the FDA had rushed its approval of the drug in 2000 without adequate scientific evidence of the drug’s safety and that the medication was dangerous. Lower courts upheld these claims, but the Supreme Court stayed these rulings and agreed to hear the case.
Meanwhile, the Biden administration filed a lawsuit against Idaho, challenging the state’s total ban on abortion as a violation of the Emergency Medical Treatment and Active Labor Act (EMTALA), which required states receiving Medicare funding to provide emergency medical care to patients, including abortion health care if necessary to stabilize a patient.
In June 2024, just months before a presidential election, the Supreme Court punted on both cases, ruling that the plaintiffs in the mifepristone case lacked standing and that they had “improvidently granted” review of the EMTALA case. These rulings left the underlying issues unresolved.
At the state level, abortion rights supporters challenged abortion bans under state constitutions and organized for ballot measures to establish abortion rights. Abortion advocates in Michigan, for example, filed a legal challenge to the state’s pre-Roe ban on abortion. In September 2022, a Michigan court ruled that the state’s abortion ban violated women’s equal rights, bodily integrity, and dignity under the Michigan Constitution.
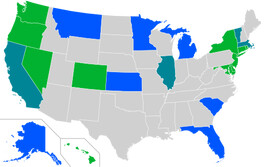
Between June of 2022 and November of 2023, seven states had abortion-related ballot measures. In all seven states, voters chose to protect abortion rights. In August of 2022, voters in Kansas rejected an anti-abortion measure by 59 to 41. That November, voters overwhelmingly supported constitutional amendments to guarantee abortion rights in California (67 to 33), Michigan (57 to 43), and Vermont (77 to 23), while voters rejected anti-abortion ballot referenda in Kentucky (52 to 48) and Montana (53 to 47). In November 2023, voters in Ohio voted 57 to 43 in favor of a constitutional amendment protecting abortion rights. In the November 2024 election, ten states had ballot measures to enshrine abortion rights in state constitutions, including Arizona, Colorado, Florida, Maryland, Missouri, Montana, Nebraska, Nevada, New York and South Dakota—the highest number of abortion ballot measures in a single year on record. In only one state, Nebraska, was there an anti-abortion ballot measure.
Support for Self-Managed Abortions
As abortion bans and restrictions went into effect after Dobbs, a movement emerged to help people learn to self-manage an abortion.
Reproductive health advocacy organizations like Aid Access, Plan C, and Women Help Women provided information and support on how to safely obtain and use abortion pills. Community groups, many affiliated with Red State Access, formed to provide free abortion pills to people living in states with bans. Between August 2022 and August 2024, these community groups provided free abortion pills to 70,000 people. These groups also offered doula support, either in person or virtually by phone, text or email. They also provided detailed information about how to use the pills by email and they ensured that people were within thirty minutes of emergency care in the rare event that they needed it.
When some states prosecuted people who obtained and used abortion pills, the legal advocacy organization If/When/How: Lawyers for Reproductive Justice pushed for the decriminalization of self-managed abortion. If/When/How also provides legal information to people with questions about self-managed abortion and their rights.
Trump Re-Elected, Abortion Rights Further Endangered

{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
On November 6, 2024, Americans elected Donald Trump for a second term, opening the door to further restrictions on reproductive rights. The MAGA Republican agenda, Project 2025, calls on the next president to direct the Food and Drug Administration to reverse approval of the abortion pill mifepristone and to ban telehealth abortion. It also directs the Department of Justice to misuse an 1873 anti-obscenity law, the Comstock Act, to criminally prosecute anyone who mails abortion pills and potentially any medical instrument used in procedural abortion. This application would effectively establish a nationwide ban on abortion.
On abortion funding, Project 2025 calls for the reimposition of the domestic gag rule that bars reproductive health clinics receiving Title X funding from mentioning abortion or referring patients for abortion care. Project 2025 also calls for the withdrawal of Medicaid funds from states that require insurance coverage for abortion and it would require states to track and report all abortions to the federal government.
Conclusion: Abortion is a Human Right

Access to safe and legal abortion is vital to women’s health and well-being. In 2020, Dr. Diana Greene Foster published the results of an extensive 10-year study, The Turnaway Study: Ten Years, A Thousand Women, and the Consequences of Having — or Being Denied — an Abortion. The research provides definitive evidence that access to abortion strongly enhances women’s mental health, physical health, and socioeconomic status. Women who were denied access to abortion and carried an unwanted pregnancy to term were more likely to experience worse outcomes.
International bodies, including the United Nations and the World Health Organization, have recognized abortion and other reproductive rights as human rights under international treaty law. As new generations of activists take on the fight, advocates, activists, and voters will continue to strive for a world where all people have access to safe and legal abortion care.
